IBS. Three letters that millions of people across India get handed after months of tests, multiple specialists, and no real answers. Irritable bowel syndrome. It sounds like a proper diagnosis, and most patients walk out of the clinic believing they finally have one.
But here is what most people are never told: IBS is not a diagnosis in the way that piles, gallstones, or appendicitis is a diagnosis. It is an umbrella term for a collection of gut symptoms that do not have a single cause. It tells you what the gut is not doing right. It does not tell you why.
This is the core reason IBS treatment in India fails so often. Patients with completely different underlying gut problems are grouped together and given the same treatment plan. One size fits all. And for most of them, it does not fit at all.
IBS affects roughly 1 in 7 adults in India. Most of them are treated as one group. Most do not get significantly better because they are not one group.
After seeing thousands of patients at Gut Care Clinics with abdominal pain, loose motions, chronic bloating, and normal investigation reports, the single biggest shift in how we approach these cases is this: we stop asking whether someone has IBS, and we start asking which pattern of gut dysfunction is driving their symptoms. That question changes the diagnosis. It changes the treatment. It changes the outcome.
Why the IBS label alone is not enough
IBS belongs to a category now officially called disorders of gut-brain interaction, or DGBI. This is an internationally recognised classification that includes more than 30 functional gut conditions, all defined by how the gut behaves rather than what it looks like on a scope or scan.
The Rome IV criteria, the international gold standard for classifying these conditions, make it clear that patients sitting under the IBS umbrella can have vastly different mechanisms driving their symptoms. One patient’s gut moves too slowly. Another’s fires too fast. One has hypersensitive gut nerves. Another has a bacterial imbalance in the small intestine. A fourth has a hormonal trigger. All four get told they have irritable bowel syndrome. All four need a different treatment plan.
This is not a failure of medicine. It is a failure of the consultation time most doctors have available. A proper pattern assessment takes 30 to 45 minutes. Most IBS consultations in India take three.
If you have been searching for terms like stomach pain after eating, loose motions every morning, chronic bloating despite normal reports, or IBS treatment that is not working, this is the reason, and this article is written for you.
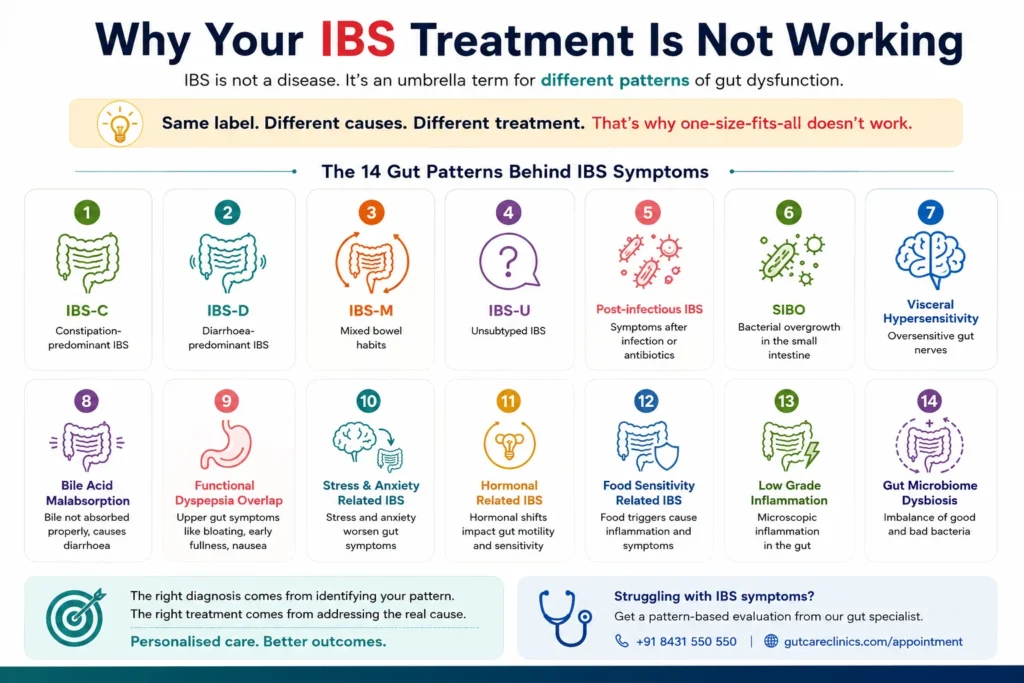
The 14 gut patterns behind IBS symptoms
These are not invented subcategories. They are drawn from Rome IV clinical classification, from published Indian gastroenterology consensus guidelines, and from what we see consistently in our Bengaluru practice. Identifying the correct pattern is what makes treatment work.
Pattern 1: IBS-C — constipation-predominant IBS
Fewer than three bowel movements a week, hard or lumpy stools, a persistent feeling that the bowel has not fully emptied. The gut is moving too slowly. This is one of the most searched gut conditions in India among women over 30. Laxatives alone rarely solve it because the root issue is gut motility, not just stool texture.
Pattern 2: IBS-D — diarrhoea-predominant IBS
Loose or watery stools on more than 25 percent of days, urgency that disrupts work and social life, abdominal cramping that sometimes resolves after passing stool. IBS-D is one of the top searched gut health symptoms in India. It is also one of the most underdiscussed because the urgency and unpredictability stop patients from even describing it fully in a three-minute consultation.
Pattern 3: IBS-M — mixed bowel habits
The most confusing pattern for patients. Constipation for several days followed by sudden loose motions. This switching pattern leads many people to try remedies for one condition and inadvertently worsen the other. IBS-M needs an approach that does not aggravate either end of the spectrum, which is why generic treatment almost always falls short.
Pattern 4: IBS-U — unsubtyped IBS
Symptoms clearly meet the IBS criteria but do not fall neatly into C, D, or M. Often seen in the early stages of the condition or when dietary changes have made the stool pattern inconsistent. Still needs proper pattern assessment, not a wait-and-watch approach.
Pattern 5: Post-infectious IBS
This pattern follows a gut infection, a course of antibiotics, or a severe episode of food poisoning or traveller’s diarrhoea. The infection resolves. The gut never fully resets. Given how frequently gut infections occur in Indian cities, this is one of the most underdiagnosed patterns in the country. Patients often present years after the original infection with symptoms they cannot trace to any clear cause. Treatment must address the disruption caused by that original event.
| Gut symptoms that started after a bad stomach infection or antibiotic course? Post-infectious IBS is treatable. Call +91 8431 550 550 or book at gutcareclinics.com/appointment. |
Pattern 6: SIBO — small intestinal bacterial overgrowth
SIBO is among the most frequently missed causes of severe chronic bloating and gas in India. Bacteria that belong in the large intestine migrate to the small intestine and ferment carbohydrates before they are absorbed. The result is pronounced bloating after meals, significant gas, and unpredictable bowel habits that do not respond to standard IBS treatment. A specific breath test identifies it. A specific treatment course resolves it. Many patients who have searched why is my bloating not going away or bloating after every meal India and found no answers have undiagnosed SIBO.
Pattern 7: Visceral hypersensitivity
The gut’s nerve endings become oversensitive. Pressures and movements that a normal gut registers as nothing produce real, measurable pain. This is not anxiety. This is not in the patient’s head. It is a documented physiological change in how gut nerves fire, and it explains the most common complaint we hear: abdominal pain with no cause found on any investigation.
Pattern 8: Gut-brain axis dysregulation
The gut has its own nervous system, and it runs a constant two-way conversation with the brain. Chronic stress, poor sleep, irregular meal timings, and high-pressure work schedules, all extremely common among urban professionals in Bengaluru, Delhi, and Mumbai, disrupt this pathway. The result is real, physical gut symptoms. Gut-brain axis dysfunction is a legitimate medical mechanism, not a polite way of saying the problem is psychological.
Pattern 9: Functional dyspepsia overlap
A significant number of IBS patients also have functional dyspepsia, where the stomach empties too slowly. This produces early fullness after small amounts of food, nausea, upper abdominal discomfort, and bloating that begins well before the intestine is involved. When both patterns are present and only one is treated, patients improve partially but never fully. Acid reflux and GERD sometimes coexist with this pattern as well.
Pattern 10: Gut microbiome imbalance
A sustained shift in the balance of gut bacteria, often driven by repeated antibiotic use, highly processed diets, chronic irregular meal patterns, or long-term stress, changes how the gut handles fermentation and regulates inflammation. This is distinct from SIBO and needs a different intervention. Probiotic supplements bought at a pharmacy without identifying the specific imbalance rarely correct it.
Pattern 11: FODMAP-triggered gut reactivity
Not an allergy. Not a classic food intolerance either. Certain fermentable carbohydrates called FODMAPs trigger excessive fermentation and symptom flares in a large proportion of IBS patients. The challenge in India is that a proper low-FODMAP trial needs to be designed around Indian food. Telling a Kannadiga or a Tamil family to eliminate onion, garlic, and dal simultaneously without guidance is not a low-FODMAP trial. It is a recipe for failure. A dietitian who understands Indian eating patterns makes this intervention actually work.
Pattern 12: Hormonal gut pattern
Thyroid dysfunction directly alters gut motility. Hypothyroidism slows the entire gut down and is one of the first things we check in patients with chronic constipation and no other clear cause. Hyperthyroidism speeds the gut up. In women, hormonal shifts across the menstrual cycle and into perimenopause produce documented changes in bowel behaviour. This pattern is consistently missed when only the gut is investigated.
Pattern 13: Pelvic floor dysfunction
This pattern is common, significantly undertreated, and almost never discussed openly. When the pelvic floor muscles fail to coordinate properly during defecation, patients experience chronic constipation, incomplete emptying, straining, and sometimes pain. It presents identically to IBS-C but does not respond to laxatives, fibre supplements, or dietary changes. It requires targeted physiotherapy from a specialist who works specifically with pelvic floor conditions.
Pattern 14: Centrally mediated abdominal pain
In this pattern, the central nervous system itself amplifies pain signals coming from the gut. There is no structural problem and no localised intestinal issue. Pain is persistent, sometimes widespread, and does not follow a predictable meal or bowel pattern. This falls between the gastroenterologist, the neurologist, and the pain specialist, which is exactly why it so rarely gets properly treated in India. It needs a coordinated, multidisciplinary approach.
What identifying the right pattern actually changes
When patients come to Gut Care Clinics in Indiranagar after years of failed IBS treatment across multiple cities and specialists, the most common reason treatment has not worked is that the underlying pattern was never identified. They were given a category label and a generic treatment for that category. Not a plan built around their specific gut.
Pattern identification changes which medications are appropriate. It changes which dietary adjustments are relevant and which are a waste of effort. It tells us whether a microbiome intervention, a breath test for SIBO, a hormonal screen, or a pelvic floor assessment is the right next step. It also tells us what is not worth doing, and in India, where patients are routinely sent for a fourth or fifth colonoscopy, that clarity alone saves money, time, and a great deal of anxiety.
The question is not whether you have IBS. The question is which of the 14 patterns is driving your symptoms. That answer is what determines your treatment.
If you have been living with stomach pain with no diagnosis, bloating that nothing fixes, loose motions or constipation that comes and goes, or IBS symptoms that returned after antibiotics or a stomach infection, a proper pattern assessment is the starting point for a treatment plan that can actually work.
| If your gut symptoms have never been properly explained, speak with our team. Gut Care Clinics, Indiranagar, Bengaluru. Call +91 8431 550 550 | gutcareclinics.com/appointment. |
Reviewed by the clinical team at GutCare Clinics, Bengaluru.


